

The educational materials are designed to enhance healthcare professionals’ awareness on diagnostic and drug delivery and to better understand the risks of injuries from sharp objects. By using these resources, you will gain essential insights that can enhance safety and efficiency in your work.
Explore the materials created for you to support your professional growth and improve your daily practices.

Self-Monitoring of blood glucose – Finger pricks rotation and alternate site testing
Self-monitoring of blood glucose is a part of everyday life for millions of people living with diabetes. This material presents ways to reduce the discomfort associated with fingertip blood sampling and introduces the option of using Alternate Site Testing (AST).
Safety lancets lancing procedure and lancing technique
This material presents the capillary blood lancing procedure and technique recommended by HTL-STREFA, confirmed by the results of clinical studies. This clinically proven lancing procedure increases the expected blood volume while simultaneously reducing pain perception.

HTL-STREFA injection technique recommendations
Proper injection technique helps people with diabetes get the best health results by delivering the right dose of insulin to the correct site with the proper needle size. For your safety and convenience, we prepared a short guide to improve insulin delivery and make daily life easier.
HTL-STREFA coloring pages – part 1, diabetes
The first part of a coloring book series that helps children understand diabetes. Meet Ann, a young girl living with diabetes. In the first part, you’ll learn how she was diagnosed and what her daily life is like. Through illustrations, discover how Ann manages her diabetes with courage and support of loved ones.
HTL-STREFA coloring pages – part 2, how to inject insulin?
The second part of a coloring book series that helps children understand diabetes. In this part, Ann shows how she takes insulin. Through engaging illustrations, children learn about insulin injections and why they are important for Ann’s health.
HTL-STREFA coloring pages – part 3, pen needles – single use only
The third part of a coloring book series that helps children understand diabetes. In this part, Ann explains why, for safety reasons, insulin pen needles should only be used once. Through illustrations, children learn about proper needle use and why it’s important to change the pen needle after each injection.
HTL-STREFA coloring pages – part 4, blood glucose monitoring
The fourth part of a coloring book series that helps children understand diabetes. In this part, Ann explains step by step how to measure blood sugar levels and why she does it every day. Through engaging illustrations, children learn about the importance of regular blood sugar monitoring to stay healthy.

Diabetes and travel
When you have diabetes, vacation or business trips require a little extra planning. Changes in what you eat, how active you are, and time zones can affect your blood sugar levels. In this brochure, you will find recommendations on how to prepare for a trip.

Diabetes and hot weather
This brochure provides essential tips for staying safe in hot weather if you have diabetes. It includes information on staying hydrated, properly storing medications, and other important precautions. Learn how to manage your condition and protect yourself during heatwaves.
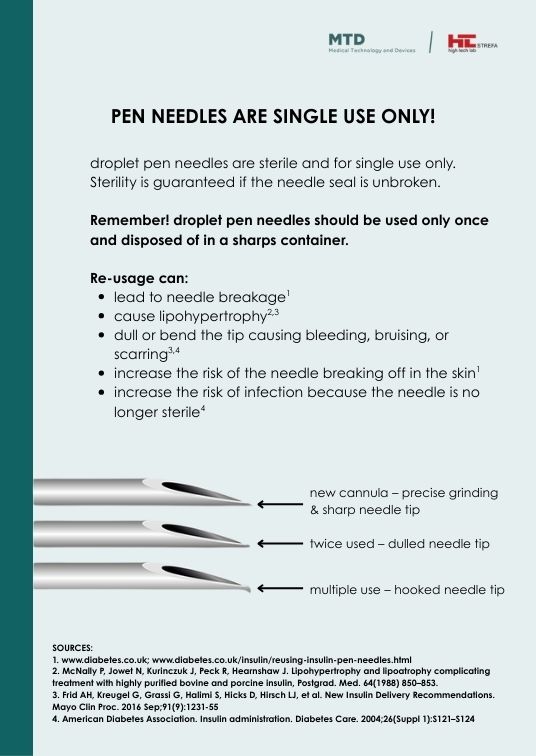
Pen needles are single use only
This leaflet explains why Droplet pen needles are for single use only. Reusing them can cause infections, skin damage, and even needle breakage inside the body.
Safe and effective use of a passive safety needle by healthcare professionals in a simulated environment, including perceptions and preferences
Needlestick injuries pose a serious risk to healthcare workers, prompting the development of a new passive safety needle. A simulated study showed that it can be used safely and effectively, offering improved protection against NSIs compared to existing solutions.
Blood volume and pain perception during finger prick capillary blood sampling: are all safety lancets equal?
The study aimed to compare different types of safety lancets in terms of capillary blood volume and pain perception during routine fingerstick sampling. Results showed that blade-type lancets produced higher blood volumes than needle-type devices but were generally associated with greater pain intensity.
Capillary blood sampling procedure in pediatric population
Capillary blood sampling from the heel is a routine procedure performed in newborns to collect samples for screening tests that require small but accurate blood volumes. The effectiveness and safety of this method depends on proper puncture technique and site selection, as defined in clinical guidelines, to minimize pain and tissue damage.
Capillary blood sampling in adults
Capillary blood sampling is a widely used, simple, and effective method for early disease detection and routine health monitoring. In adults, it involves a finger prick and is valued for its speed, low cost, and broad accessibility in both outpatient and clinical settings.
Evaluation of three lancing devices: what do blood volume and lancing pain depend on?
Millions of people with diabetes worldwide still perform finger pricks to measure blood glucose levels. This study compared three common lancing devices at minimum and maximum depth settings, showing that puncture depth significantly affects both blood volume and pain, with some influence from the device type on pain perception.
Dropsafe safety pen needle helps to prevent accidental needlesticks after injections: results of a simulated clinical study
DropSafe safety pen needle was designed to prevent accidental needlestick injuries, a persistent risk during injection procedures. A simulated study confirmed the effectiveness of its safety mechanism and ease of use, supporting its suitability for both healthcare professionals and non-clinical users.
A single-blind, randomized, single-centre study to investigate the characteristics of different personal lancets on blood volume and perceived pain in patients with diabetes mellitus
This randomized clinical trial evaluated the effectiveness and comfort of various personal lancets in patients with diabetes. Results confirmed that Droplet® 33G and Glucoject® 33G lancets provide sufficient blood volume for glucose testing with minimal pain perception.
The impact of needle diameter and penetration depth of safety lancets on blood volume and pain perception in 300 volunteers: a randomized controlled trial
This study assessed blood volume and pain levels after lancing with various safety lancets in 300 volunteers. Findings showed that all tested devices are effective and safe, with thicker needles producing higher blood volumes while maintaining low pain levels.